Advertisement
A 43-year-old’s childhood pectus excavatum repair demands revisiting
A recent case managed in Cleveland Clinic’s Section of Thoracic Surgery underscores the need for vigilance for acquired thoracic dystrophy when an adult with childhood pectus excavatum repair presents with exercise intolerance. This article recaps the case details and presents a Q&A with the managing thoracic surgeon, Daniel Raymond, MD, on insights to be gleaned about this rare condition.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 43-year-old male presented to Cleveland Clinic’s Center for Chest Wall Disease with significant exercise intolerance. He was very short of breath and limited in his daily activities. Attempts to exercise led to palpitations and profuse sweating. On cardiopulmonary testing, his maximal oxygen uptake (VO2max) was 42 percent of predicted.
At age 7 years, he had undergone a modified Ravitch procedure to correct a pectus excavatum defect, which entailed removal of the cartilage between the sternum and ribs. In his case, this procedure had resulted in destruction of the growth plates so that his ribs had stopped growing. This essentially had left him with the rib cage of a 7-year-old with adult-sized organs squeezed within.
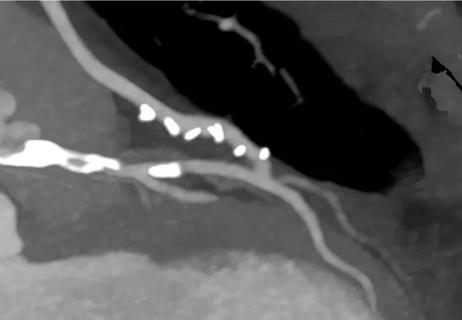
The clinicians he had seen previously believed he had a recurrence of the pectus excavatum, as his sternum looked low on imaging, as if the defect had perhaps not been corrected entirely. However, CT scans at Cleveland Clinic revealed the telltale sign of acquired thoracic dystrophy: a bell-shaped chest (Figure 1) associated with a restrictive pattern on his lung function studies. Moreover, axial images showed his organs to be visibly crowded in the chest (Figure 2), restricting space for his lung tissue. In addition, the normal cartilage between his ribs had been replaced by bone, reducing his chest wall flexibility.

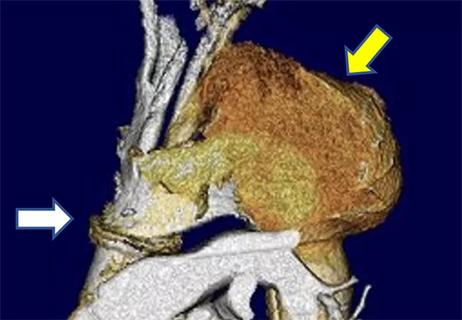
Figure 1. Preoperative image showing the classic bell-shaped chest of acquired thoracic dystrophy.

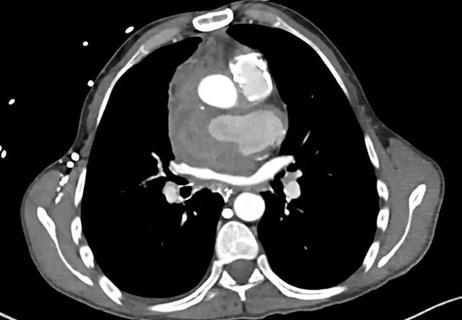
Figure 2. Preoperative axial image showing calcification of the medial ribs with some residual pectus deformity.
The patient was operated on at Cleveland Clinic in November 2017. We resected the rib portions that had calcified, taking care to preserve the soft tissue underneath. We then cut his sternum and bent it forward since there was still a residual component of his pectus excavatum. Next we inserted a titanium plate to hold his sternum in its new, normal position.
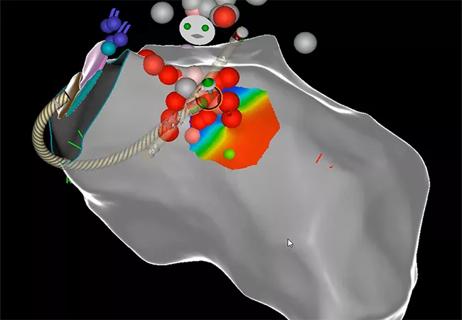
Because his organs were so restricted, we also used a bar to cross his chest and push the sternum forward to create even more volume in the chest (Figure 3). We generally avoid use of bars in adults when correcting previously untreated pectus excavatum, but in this case the patient’s need for additional chest wall expansion was clear. We plan to remove the bar in or about November 2019, after the patient has had it in for two years. The plate will remain permanently.

Figure 3. Postoperative image showing the plate and bar placed to hold the sternum in its normal position and further increase chest volume.
Q: How has the patient fared in the year or so since the operation?
Dr. Raymond: He has worked very hard at exercising and has improved dramatically. On repeat cardiopulmonary testing, his VO2max is now up to 78 percent of predicted. This is due not simply to the surgery but also to his hard work: He walks every day, goes to the gym and does all the exercise we prescribed for him. Since he has been able to exercise, he has lost about 30 pounds as well.
Advertisement
While we made his chest wall better, the patient had to be the one to improve his own cardiopulmonary fitness. Unfortunately, many patients don’t do that. He is unlikely to have had such a positive result without this dedication to improving his status.
Interestingly, despite the improvement in VO2max, his forced vital capacity and forced expiratory volume at one minute have not changed dramatically since the surgery, remaining at about 50 percent. We do not currently have effective technology to surgically increase the thoracic cage volume to a significant degree, and this offers an opportunity for research.
Q: Exactly how can a modified Ravitch procedure for pectus excavatum in childhood contribute to development of acquired thoracic dystrophy?
Dr. Raymond: Pectus excavatum is a congenital chest wall deformity in which several ribs and the sternum grow abnormally, producing a concave appearance in the anterior chest wall. It is fairly common, occurring in about 1 in every 300 births, with a male:female dominance of about 3:1.
In most cases, the defect is mild and doesn’t require correction, although sometimes in children cosmetic treatment is justified for psychological reasons. In adults, we do not correct pectus excavatum unless there are problems with exercise intolerance, which can be overlooked. Patients are often told that pectus excavatum is only a cosmetic problem when in fact there can be real physiologic manifestations.
Advertisement
In the mid-1980s, the pediatric surgical community recognized that pectus excavatum could be corrected without damage to the growth plates, by being less aggressive in dissecting the interface between cartilage and bone. The modified Ravitch is still used, but a newer, less invasive approach called the Nuss procedure has largely replaced it.
With the Nuss, the cartilage stays in place while a bar is pushed under the sternum to force it forward. While the Nuss works well in children and teens, it tends to be more painful than the Ravitch. My practice is to not perform the Nuss in adults out of concern that rigidity of the adult skeletal system leads to rib fractures without effective correction of the defect. However, other surgeons will perform the Nuss procedure in adults.
Q: Does this mean acquired thoracic dystrophy will disappear as a clinical entity?
Dr. Raymond: Current awareness of the need for greater care in cartilage dissection with the modified Ravitch, along with the elimination of dissection altogether with greater use of the Nuss, means that we should be seeing fewer and fewer cases of ATD as time goes by. But we can’t predict when we’ll stop seeing them, since we don’t know how many cases are out there.
Q: What’s needed for the management of restrictive chest wall diseases like this?
Dr. Raymond: At Cleveland Clinic’s Center for Chest Wall Disease, we are fortunate to be able to pool the expertise of thoracic surgeons along with clinicians in orthopaedics, radiation oncology, musculoskeletal radiology, pulmonary physiology and pain management to help these patients. We are now working on developing new technologies to more effectively expand the chest volume to treat acquired thoracic dystrophy as well as other restrictive diseases.
Advertisement
Advertisement

Excessive dynamic airway collapse presenting as dyspnea and exercise intolerance in a 67-year-old
Young man saved multiple times by rapid collaborative response
Necessity breeds innovation when patient doesn’t qualify for standard treatment or trials
After optimized medical and device therapy, is there a role for endocardial-epicardial VT ablation?
Fever and aortic root bleeding two decades post-Ross procedure

How to time the interventions, and how to manage anesthesia risks?

A potentially definitive repair in a young woman with multiple prior surgeries
Matching the minimally invasive CABG alternative to the right candidates